-
Address:
17888 67th Court North
Loxahatchee, FL
-
Mail us:
contact@wrightacademia.org
- submit manuscript
Case Report |
Open Access |
Volume 1 | Issue 1 |
Lower Extremity Disarticulation and Extended Total Thigh Flap for Complex Repair of an End Stage Pressure Ulcer in a Spinal Cord Injury Patient
Lynn M Frydrych, MD1, Andrea Zaw, MD2, Salah Rubayi, MD, FACS2
1Division of Plastic Surgery, Department of Surgery, University of California, Los Angeles, USA
2Department of Surgery, Rancho Los Amigos National Rehabilitation Center, USA
*Corresponding author: Salah Rubayi, MD, FACS, Department of Surgery, Pressure Ulcer Management Program, Rancho Los Amigos National Rehabilitation Center, Downey, CA, USA, E-mail: srubayi@dhs.lacounty.gov
Citation: Frydrych LM, Zaw A, Rubayi S (2021) Lower Extremity Disarticulation and Extended Total Thigh Flap for Complex Repair of an End Stage Pressure Ulcer in a Spinal Cord Injury Patient. J Surg Clin Rpts 1:004.
Copyright © Frydrych LM, et al.
Received: |
Accepted: |
Published: |
Pressure injuries are the result of unrelieved pressure leading to localized ischemia. This leads to cell death and tissue necrosis. One in three spinal cord injury patients are affected by pressure injuries, likely secondary to the fact that these patients have 3 major risk factors for the formation of pressure injuries-loss of sensory perception, loss of motor function, and moisture from bowel and bladder incontinence. When non-operative local wound care fails, surgical wound debridement and vascularised soft tissue reconstruction is required to manage the pressure wounds. In recurrent or extensive pressure wounds, exhaustion of available tissue flaps occurs. Lower extremity disarticulation and total thigh flap is an end-stage reconstructive procedure for patients with extensive pressure ulcers, when all other available flap options have been exhausted. On occasion, the standard total thigh flap, where the amputation is above the knee, is too short and cannot reach and cover the full extent of the wound. In this instance, an extended total thigh flap, where extra length is obtained from the posterior leg muscle compartments and overlying skin, can be used. This case report describes a paraplegic patient with a T10 complete spinal cord injury with extensive Stage IV pressure ulceration of the bilateral posterior thighs, perineum, and coccygeal area with exposed perineum, urethra, and left femur requiring left lower extremity disarticulation and extended total thigh flap.
Introduction
Pressure injuries are wounds caused by unrelieved pressure leading to local ischemia. Depending on the duration of pressure, the affected skin and soft issue will experience anoxia, ischemia, and eventually necrosis and irreversible tissue damage [1]. The main etiologic factors leading to the development of such injuries including pressure, shearing forces, friction, and moisture [2]. Pressure injuries are staged according to the extent of tissue damage. The National Pressure Ulcer Advisory Panel (NPUAP) redefined the definitions of pressure injuries in 2016. Stage 1- Intact skin with a localized area of non-blanch able erythema, Stage 2- Partial thickness skin loss with exposed dermis, Stage 3- full thickness skin loss with exposed adipose tissue, and Stage 4- Full thickness skin and tissue loss with exposed or directly palpable fascia, muscle, tendon, ligament, cartilage or bone. If slough or eschar obscures the extent of full-thickness skin and tissue loss, it is classified as an Unstageable Pressure Injury [3].
Individuals with normal sensation, mobility, and mental status generally do not suffer from pressure injuries, as prolonged pressure elicits a feedback response that prompts a change in body position [4]. If this feedback response is altered, such as in immobile, insensate patients, one's risk of developing pressure injuries increases. Spinal cord injury patients are disproportionately affected by pressure injuries. This is because they have three major risk factors for the formation of pressure injuries - loss of sensory perception, loss of motor function, and moisture from bowel and bladder incontinence [5]. A recent systematic review and meta-analysis revealed that about one in three patients with spinal cord injury had pressure ulcers [6]. The psychological, physical, and social burden of these injuries not only decreases the quality of life of these patients, but also substantially impacts the health care system, [6] as individuals with pressure injuries have recurrent hospitalizations, surgeries, clinic visits, and home healthcare needs [7]. Additionally, pressure injuries can be life-threatening in end-stage cases as they can lead of overwhelming sepsis and have complications from osteomyelitis, joint destruction, muscle and soft tissue necrosis, and erosion into neigh boring vital structures [7].
Therefore, once a patient develops a pressure ulcer, immediate treatment is recommended. The treatment depends on the severity of the ulcer. Stage I and II pressure injuries can usually be treated with non-operative local wound care, while Stage III and IV ulcers will commonly require surgical treatment, including complete wound excision, including debridement of colonized and osteomyelitic bone, and vascularized soft tissue reconstruction [7]. Both non-operative and operative treatment strategies should incorporate pressure redistribution therapy, nutrition optimization, ulceration precautions, and patient/caretaker education to manage the current ulcer and prevent new ulcers and/or recurrence [5,7]. Here we present a case of extensive Stage IV ulceration of the bilateral posterior thigh, perineum, and coccygeal area with exposed perineum, urethra, and exposed left femur requiring left hip disarticulation and extended total thigh flap for reconstruction.
Case Presentation
Clinical history
The patient is a 48-year-old male with T10 complete spinal cord injury secondary to a gunshot wound almost 30 year prior and past medical history including neurogenic bowel and bladder secondary to his spinal cord injury, hypertension, dyslipidemia, and type 2 diabetes mellitus. His surgical history included open left nephrectomy and previous colostomy, now closed. When our team met the patient in the outpatient clinic, he had a large 15 cm × 10 cm Unstageable pressure injury of the sacrum and bilateral ischia enveloping the anus and a 2 cm × 3 cm Stage III pressure injury of the left ischium, secondary to prolonged wheelchair sitting. Given the location of the injury around the anus, the constant fecal soiling was worsening the injury. Therefore, our treatment plan included local wound care and offloading while we requested fecal diversion with a loop colostomy to ensure success of any future reconstructive surgery. The patient subsequently developed an urethrocutaneous fistula that drained into the pressure ulcer, so the patient also required urinary tract diversion. Despite urgent request for both fecal and urinary diversion, these procedures were delayed due to the COVID-19 pandemic. During this time, the patient's pressure ulcers continued to be managed medically with local wound care; however, the wounds continued to evolve. Approximately 6 months after we first met the patient, he had a 7 cm × 6 cm Stage IV right ischium pressure ulcer with the ischium palpable within the wound, an 8 cm × 9 cm × 4 cm Stage IV left ischio-trochanteric pressure with lateral undermining up to 10 cm in all directions with the femur and hip bones palpable within the wound, and a 4 cm × 2 cm × 3 cm Stage IV perineal ulcer that communicated with the left ischio-trochanteric ulcer in a tunneling fashion. Given our inability to obtain fecal/urinary diversion due to the COVID-19 pandemic, surgical debridement and reconstructive surgery was subsequently delayed. We continued with medical management of his wounds.
Unfortunately, 3 months after we last saw the patient in clinic, he developed a left hip fracture with the femoral bone exposed through the left hip ulcer. He was admitted to an outside hospital. Where he was treated for sepsis secondary to the infected pressure ulcers and underwent an unknown failed flap surgery closure. He had yet to receive fecal or urinary diversion prior to the flap surgery. We saw the patient in our clinic for follow-up, after he was discharged from the outside hospital. On clinic intake, he was noted to be tachycardic and hypotensive, with multiple ulcers that were malodorous and contained necrotic tissue. He had a Stage IV left trochanteric-ischial-perineal pressure ulcer measuring 20 cm × 20 cm × 9 cm deep, with exposed open left proximal femur fracture, necrotic bone and muscle, and perineal urethral erosionwith exposed indwelling foley catheter; a Stage IV right trochanteric-ischial-perineal pressure ulcer measuring 13 cm × 20 cm × 5 cm with exposed right proximal femur; a Stage IV sacrococcyx pressure ulcer measuring 10 cm × 20 cm × 5 cm extending to the sacral bone 1 cm from the anus; and a Stage III right heel pressure ulcer measuring 6 cm × 5 cm (Figure 1). He was immediately admitted to the intensive care unit for medical stabilization, with the plan to transfer the patient to a facility for permanent diverting end colostomy and suprapubic tube placement with bladder neck closure for fecal/urinary diversion once stable. Given how extensive his pressure ulcers now were, the local my ocutanous flaps usually utilized for closure of pressure ulcer wounds after debridement were not unavailable. Consequently, our new reconstructive plan now included the end-stage procedure of left hip disarticulation and total thigh flap after debridement of all involved soft tissue and bone, anus excision, and urethral reconstruction.
While in the intensive care unit, the patient developed a paralytic ileus requiring nasogastric tube placement and pulmonary edema secondary to heart failure of unknown etiology (presumed stress related). His medical stabilization after his initial intensive care admission took over one month. However, the patient was finally able to be transferred to another hospital and received a diverting colostomy for fecal diversion. He was then transferred back to our medical facility for further optimization prior to surgical intervention for his pressure ulcers. He received a suprapubic tube placement for urinary diversion. He received a percutaneous endoscopic gastrostomy tube for enteral nutrition to optimize his nutrition. Finally, he received pre-operative clearance by Cardiology, Pulmonology, and Anesthesia. Two and a half months after urgent intensive care admission from our clinic, and a full year after we initially met this patient, he was medically optimized and ready to undergo operative treatment of his extensive pressure ulcers. Our plan was to address the left sided proximal thigh/perineal/coccygeal ulcers during a first surgery, and then come back to address his right posterior thigh ulcer during a second surgery. In addition, during that time he had multiple bedside debridements and shortening the exposed right necrotic femoral shaft.
Operative procedure
Prior to surgery, central venous access was established through a left subclavian central venous catheter and an arterial line was placed.
The patient was positioned in the prone position after padding all bony prominences using Allevyn adhesive foam (Smith & Nephew, London, UK). The penile foley catheter was exchanged under sterile conditions, which would allow us to identify the ends of the interrupted urethra for reconstruction during the operation. Marking of the extensive ulcers to be excised was performed (Figure 1).
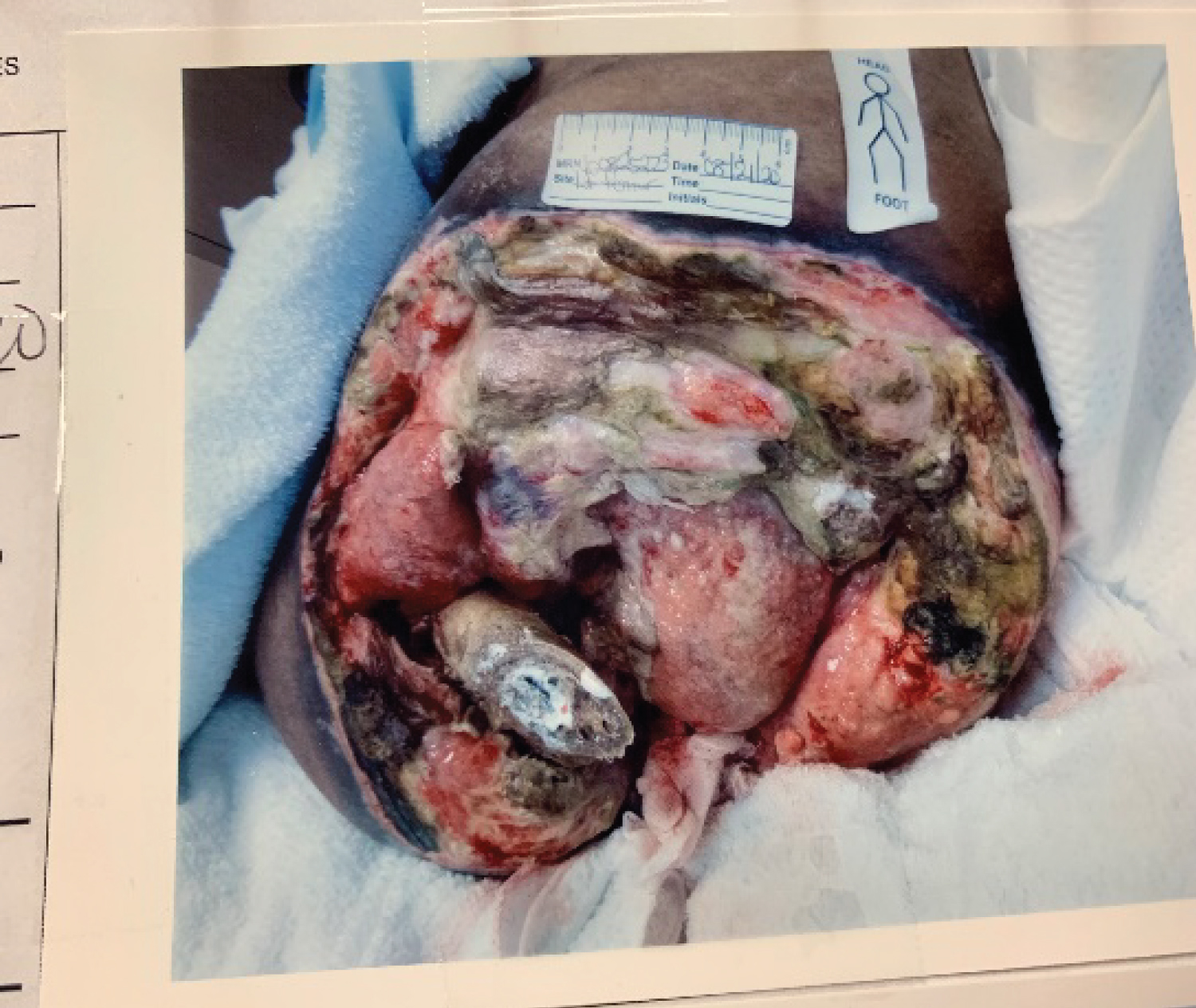
Figure 1: Extent of the pelvic ulceration and necrosis (prone position).
Given the extensive ulcers, we anticipated that a standard total thigh flap, where the amputation is above the knee, was going to provide too short of a flap for total coverage. Thus, we planned to utilize the gastrocnemius muscles and the attached skin in the posterior leg compartment to obtain more flap length, making it an extended total thigh flap. The extended total thigh flap was designed on the left leg (Figure 2, Figure 3 and Figure 4).

Figure 2: Extent of the necrosis of the right side.

Figure 3: Extent of the ulceration post local wound debridement (prone position).

Figure 4: Lateral view of the left side showing the marking for disarticulation.
We first turned our attention to excision of the ulcers. Using electrocautery, we excised all devitalized tissue associated with the left posterior thigh, perineum, and coccygeal ulcers down to the level of bone. Using a curette, the base of the wounds was debrided, and any prominent and unhealthy bone was shaved down using an osteotome and mallet. The wounds were thoroughly lavaged using 2 liters of normal saline mixed with 50,000 units of bacitracin. The excised tissue was submitted to pathology for examination.
We then turned our attention to removing the anus. A circumferential excision was designed around the anus using a skin marker. Electrocautery was used to incise the skin and dissect through the subcutaneous tissue until the serosa layer of the rectum was identified. The rectum was circumferentially dissected until approximately 6 cm of rectum was freely mobile. The rectum was clamped, the distal rectal stump/anus removed, and the rectal stump closed in a layered fashion, using a full thickness running 0 Vicryl suture (Ethicon Cincinnati, OH) and a running 0 Vicryl Lembert suture. There was some laxity in the remaining soft tissues surrounding the rectal stump, so we used a running 0 Vicryl suture to approximate the surrounding soft tissue to provide another layer of soft tissue closure over the rectal stump. The anus was submitted to pathology for examination (Figure 5).

Figure 5: Operative view post debridement in the O.R. (prone position).
We then moved to raising our left extended total thigh flap. Electrocautery was used to incise both the lateral and medial skin of the thigh and lower leg and dissect the soft tissue along our previously designed flap, from the proximal thigh down to the tibial shin where our flap then extended circumferentially above the level of the Achilles tendon. At the thigh, we approached the femoral shaft laterally. Electrocautery was used to dissect the soft tissue until the lateral aspect of the femur was reached. A bone clamp was placed over the proximal end of the femoral shaft and retracted laterally. This allowed us to use electrocautery to dissect any remaining tissue attached to the femoral shaftcircum ferentially, freeing the entire length of the femoral shaft from all of the muscle groups in the total thigh. The dissection proceeded from proximal to distal. Once our dissection reached the knee, caution was taken to dissect the soft tissues directly off of the bone to ensure that the popliteal artery was preserved, as this is our blood supply to the distal aspect of our extended thigh flap. The patella bone was identified and removed. We then continued our dissection distally, carefully dissecting the soft tissues off of both the tibia and fibula. Once the femur, tibia, and fibula were completely dissected from the surrounding tissues, the distal aspect of our muscle flap was dissected circumferentially to allow complete separation of our flap from the bones and distal foot. The knee joint capsule was removed. Hemostasis was achieved throughout the total thigh flap operative field using electrocautery and suture ligatures. The femur, tibia, fibula, and distal lower leg were submitted to pathology for examination (Figure 6 and Figure 7).

Figure 6: Left disarticulation at the hip and knee.
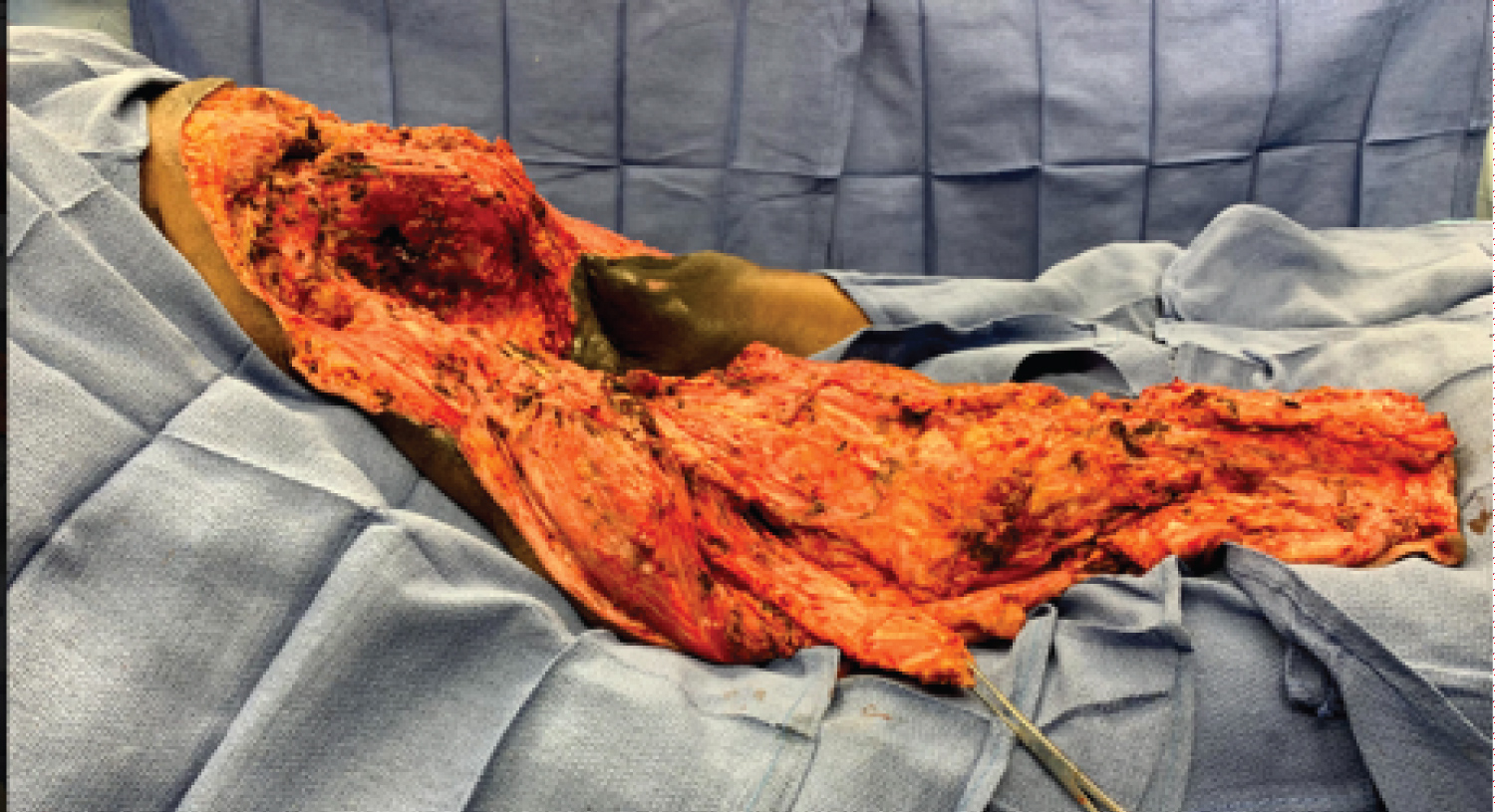
Figure 7: Post-disarticulation and total thigh flap with extension below the knee.
We then turned our attention to reconstructing the 10 cm of missing perineal urethra. The patient's previously placed Foley catheter was used to locate both the proximal and distal ends of the interrupted perineal urethra. Electrocautery was used to mobilize the soft tissue at the medial aspect of the foley catheter so that it could be reflected laterally and sutured to the lateral coccyx bone/lateral soft tissue. A running 0 Vicryl suture was used to secure this tissue over the foley catheter. Once this mobilized tissue was inset, the majority of the foley catheter was covered. There was no further soft tissue to mobilize in the area to provide further coverage.
The wounds and flap were thoroughly lavaged using 3 literrs of normal saline mixed with 50,000 units of bacitracin. Hemostasis was achieved with electrocautery. We then moved to planning the insetting of our muscle flap. Once we folded the extended thigh muscle flap proximally, we realized that the flap had enough length to not only adequately cover the debrided left thigh/coccygeal/perineal ulcers, but that it would also reach to cover the right posterior thigh ulcer. Given this extra length, we decided to move forward with debridement of the right posterior thigh ulcer so that the patient's reconstruction could be completed in a one staged approach.
Using electrocautery, we excised all devitalized tissue associated with the right posterior thigh ulcer. After debridement, there was a small bridge of skin between the left and right sided surgical wounds. This skin bridge was excised to create one continuous wound. An osteotome and mallet was used to shave down the prominent pelvic bone and rasping was completed on all exposed bone edges (Figure 8). The K-wire pointing to the sight of anal closure.
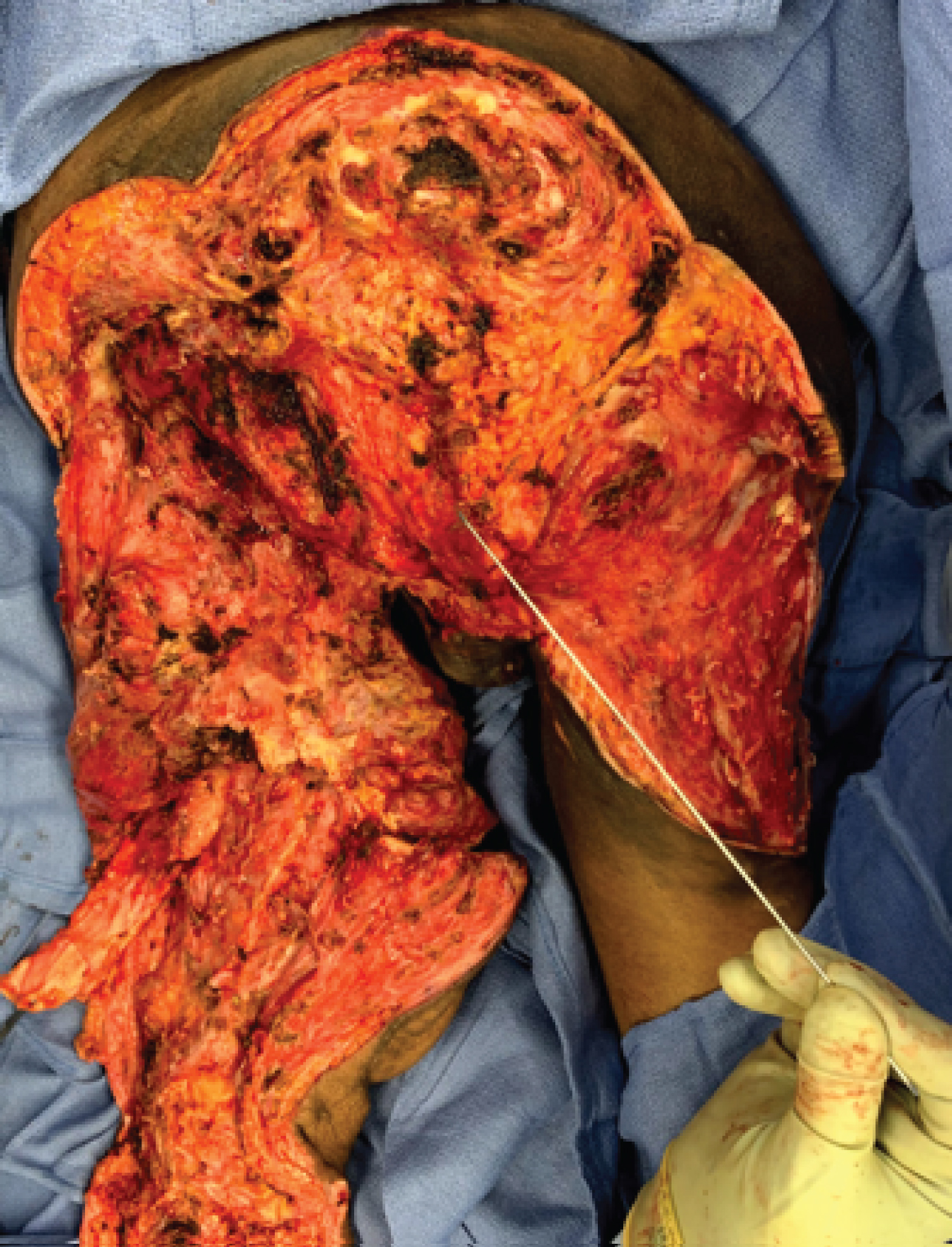
Figure 8: Operative view post-disarticulation K-wire indicate the excision of the anus and rectal closure and repair of the perennial urethra.
The wounds were thoroughly lavaged using 2L of normal saline mixed with 50,000 units of bacitracin. The excised tissue was submitted to pathology for examination. Soft tissue hemostasis was achieved with electrocautery and Avitene (Davol, Warwick, RI) was placed within the wound bed for hemostasis.
Now that our debridement was complete and we knew the full extent of our surgical wound, we once again turned our attention back to insetting the muscle flap. We identified an isolated thigh muscle approximately half-way down the muscle flap and dissected this proximally. We would use this muscle to cover our previous urethral repair (Figure 9a and Figure 9b).
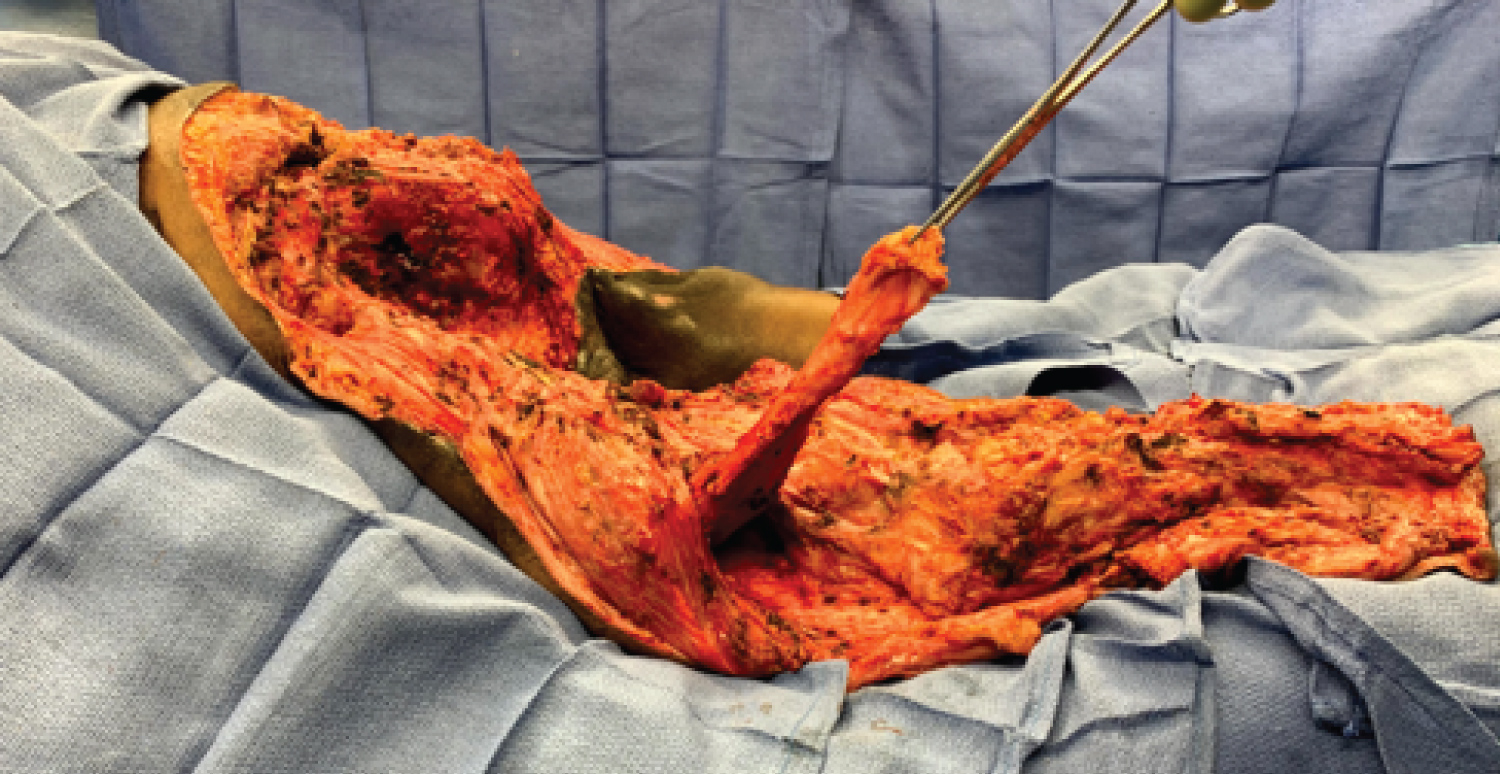
Figure 9a: Operative view post-disarticulation and utilization of the rectus femoris muscle to cover the perennial urethra repair.
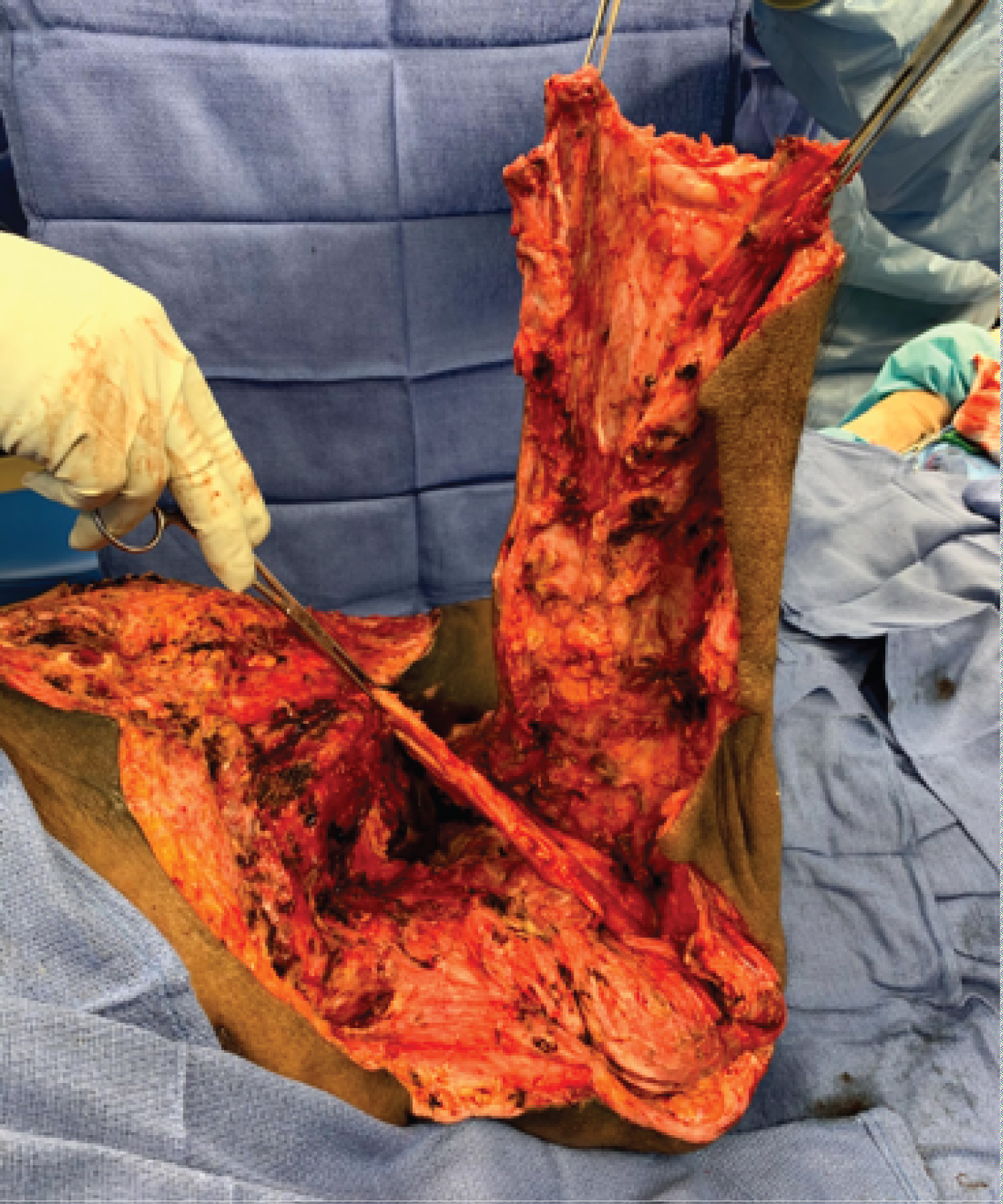
Figure 9b: Operative view post-disarticulation and utilization of the rectus femoris muscle to cover the perennial urethra.
We then placed three Shirley sump drains into the wound, all terminating within the wound bed, two exiting the left buttock and one exiting the right buttock. We then folded the muscle flap proximally. We positioned the previously isolated thigh muscle directly over our previous urethral repair and secured it circumferentially using interrupted and running 0 Vicryl sutures. The right-sided Shirley sump drain was positioned underneath this muscle flap so that we would be able to identify a urinary leak. The flap was then positioned to adequately cover the wound in its entirety and 0 Nylon retention sutures were used to secure the flap into place.
The flap was then closed in a multilayer fashion. The deep muscle and soft tissue layers of the flap were closed using a series of interrupted 0 Vicryl sutures. A running 0 Vicryl was used for a deep dermal layer. The skin was then re-approximated with a running cuticular 2-0 Monocryl (Ethicon, Cincinnati, OH) and over sewn with a running 0-Prolene (Ethicon, Cincinnati, OH) (Figure 10a, Figure 10b and Figure 10c).

Figure 10a: Operative view showing the final closure of the entire left & right side of the pelvis.

Figure 10b: Operative view showing the final closure of the entire left & right side of the pelvis.

Figure 10c: Operative view showing the final closure of the entire left & right side of the pelvis.
From the prone position, we were unable to reach the medial aspect of the wound as it was positioned too far anteriorly. Therefore, following closure of the posterior wounds, the wounds were dressed in Bactroban (GSK, Brentford, UK), Xero form (De Rroyal, Powell, TN), gauze, and abdominal pads that were silk taped in place, and the patient was then flipped to a supine position to complete closure/dressing of the anterior incision in a similar fashion as described above (Figure 11).

Figure 11: Showing complete healing of the total thigh flap about ten weeks post-surgery.
Discussion
Pressure injuries are staged according to the extent of tissue damage [3]. Staging of pressure ulcers is important for guiding treatment and determining prognosis. All treatment strategies should incorporate pressure redistribution therapy, nutrition optimization, ulceration precautions, and patient/caretaker education to manage the current ulcer and prevent new ulcers and/or recurrence [5,7]. Stage I and II pressure injuries can usually be treated with non-operative local wound care, while Stage III and IV ulcers will commonly require surgical intervention [7]. Surgical reconstruction is indicated when wounds do not heal despite medical management, which includes debridement of necrotic tissue, local wound care, control of infection and body fluid contamination, pressure offloading, and optimal nutrition [1]. Other indications for surgical wound closure include a wound that is extensive in size, or progressing in size, a wound that interferes with daily living, such as wounds that cause pain, discomfort, or disability, wounds that extend into tissue or bone causing osteomyelitis or sepsis, or extension of the pressure ulcer into vital organs [1].
When choosing the appropriate surgical technique for management of the pressure wound, many important factors need to be considered, including the patient's primary disease that contributed to ulcer formation, if it is a new or recurrent ulcer, and any prior surgical reconstructions performed [1]. Lower extremity disarticulation and total thigh flap/extended total thigh flap is an end-stage procedure for patients in which the muscle and skin reserves have become exhausted [1]. This procedure can be lifesaving for an individual who is severely disabled and would otherwise face progression of the wound, likely leading to eventual death secondary to complications from the wound.
As with all types of surgery, there can be post-operative complications. Complications specific to reconstructive flap surgery for pressure ulcer management include seroma, wound infection, hematoma, fat necrosis, and flap necrosis [1]. In most types of flap surgery, wound dehiscence is seen as a minor complication that is frequently seen, including in lower extremity disarticulation and total thigh flap/extended total thigh flap. It is not unusual to see wound dehiscence in the lower extremity disarticulation and total thigh flap/extended total thigh flap due to the heavy weight of the total thigh flap, which may predispose it to wound dehiscence [1]. However, each subsequent wound dehiscence in these complex patients creates a dilemma for repair, as anatomically there is no definite named flap to use for re-repair [1]. Nonetheless, this can be a lifesaving procedure for a complex patient, such as the one presented in this case report.
Conclusions
Spinal cord injury patients have disproportionately high rates of pressure injuries due to loss of sensory perception and motor function, and moisture from bowel and bladder incontinence. Complex pressure injuries can be life-threatening. Treatment of these injuries requires a multidisciplinary team approach, which should include a dedicated reconstructive plastic surgeon capable of performing a variety of flaps for reconstruction. When all other reconstruction options are exhausted, the lifesaving lower extremity disarticulation with total extended thigh flap provides an end-stage procedure for wound closure of extensive, complex pressure ulcers.
References
- Rubayi S (2015) Reconstructive Plastic Surgery of Pressure Ulcers.
- Kanj LF, Wilking SVB, Phillips TJ (1998) Continuing Medical Education: Pressure ulcers. J Am Acad Dermatol 38: 517-538.
- National Pressure Injury Advisory Panel.
- Mervis JS, Phillips TJ (2019) Pressure ulcers: Pathophysiology, epidemiology, risk factors, and presentation. J Am Acad Dermatol 81: 881-890.
- Christian D, Leland HA, Rubayi S (2016) Major Repair for End Stage Pressure Ulcer in a Spinal Cord Injury Patient by Disarticulation and Total Thigh Flap a Case Report. J Dermatol Plast Surg 1: 1005.
- Shiferaw WS, Akalu TY, Mulugeta H, et al. (2020) The global burden of pressure ulcers among patients with spinal cord injury: a systematic review and meta-analysis. BMC Musculoskelet Disord 21: 334.
- Kruger E A, Pires M, Ngann Y, et al. (2013) Comprehensive management of pressure ulcers in spinal cord injury: Current concepts and future trends. J Spinal Cord Med 36: 572-585.