-
Address:
17888 67th Court North
Loxahatchee, FL
-
Mail us:
contact@wrightacademia.org
- submit manuscript
Original Article |
Open Access |
Volume 2 | Issue 1 |
Epidemiological Analysis of 93 Patients with Coronavirus Disease 2019 in Jilin Province, China
Cai-Xia Liu#, Lu-Yao Sun#, Dan-Ping Peng, Yang Wang* and Kai-Yu Zhang*
Department of Infectious Diseases, The First Hospital of Jilin University, Changchun, 130021, China
*Corresponding author: Kai-Yu Zhang, Department of Infectious Diseases, the First Hospital of Jilin University, Changchun, No.1 Xinmin Street, 130021, China, Email: kaiyu@jlu.edu.cn
Citation: Liu CX, Sun LY, Peng DP, Wang Y, Zhang KY (2021) Epidemiological Analysis of 93 Patients with Coronavirus Disease 2019 in Jilin Province, China. J SARS-CoV-2 COVID 2:015.
Copyright © 2021 Liu CX, et al.
Received: |
Accepted: |
Published: |
Aim: To analyze the epidemiological characteristics of coronavirus disease 2019 (COVID-19) in Jilin Province, China.
Methods: From January 20 and February 23, 2020, COVID-19 cases diagnosed in Jilin Province, China were reviewed retrospectively. The epidemiological characteristics of enrolled cases were collected and analyzed. Descriptive statistics were computed for age, sex, source of infection (imported vs. clustered), incubation period, date of diagnosis, and case severity.
Results: A total of 93 patients were diagnosed with COVID-19 in Jilin Province over the study period. Cases included 54 males and 39 females, with a mean age of 44 years (range 7-85). The majority of patients were 20 to 59-years-old (80%, 74/93). There were 39 imported cases and 54 clustered cases. Imported cases were predominant from January 20 to 31, whereas clustered cases were predominant from February 1 to 10 and from February 11 to 23. Incubation period was accurately assessed in 40 of the 93 patients (28 males and 12 females). The median incubation period was 8 days overall (8 days in males, 11 days in females, P = 0.049). The median incubation period of clustered cases was 3 days longer than that of imported cases (10 days vs. 7 days, P = 0.061). Among the 93 patients, there were 83 mild and moderate cases, 6 severe cases and 4 critical cases. The gender distribution has no significance between them (P = 0.5797). However, age difference exist between the three groups (P = 0.0026). COVID-19 was more common in young adults than in older adults in Jilin Province, with clustered cases predominating during the later stages of the epidemic. Female patients had a longer incubation period than males.
Conclusions: Findings from this study can inform understanding of the disease transmission patterns and incubation period of COVID-19, as well as possible revisions to protocols for clinical care and observation of suspected cases.
List of Abbreviations
COVID-19: Coronavirus Disease 2019; WHO: World Health Organization; SARS-Cov-2: Severe Acute Respiratory Coronavirus 2; PCR: Polymerase Chain Reaction; SD: Standard Deviation; SARS-Cov: Severe Acute Respiratory Coronavirus; MERS-Cov: Middle East Respiratory Syndrome Coronavirus; CDC: Center for Disease Control and Prevention; CT: Computed Tomography; PLA: People's Liberation Army
Introduction
Following the discovery of a novel coronavirus disease in Wuhan City, Hubei Province, China, in December 2019, the World Health Organization (WHO) declared a public health emergency of international concern in late January 2020, and the epidemic has now spread to more than 200 countries around the world. On February 11, 2020, the International Committee of Taxonomy of Viruses officially named this novel coronavirus as severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), and the WHO introduced this new type of coronavirus infection as coronavirus disease 2019 (COVID-19) [1]. Since the outbreak of COVID-19, many provinces in China have initiated Grade I responses appropriate to a major public health emergency, including Jilin Province, which launched a Grade I response on January 25, 2020. Following a total of 93 confirmed cases over a one-month period, there have been no new local confirmed cases in Jilin since February 23, 2020, and the level of emergency prevention and control measures was adjusted to a Grade II response on February 26.
COVID-19 is now effectively under control in most provinces and cities in China, but the epidemic remains a serious challenge globally. By far apart from supportive care, no specific treatment has been established for COVID-19 [2]. Prevention is the most important means of controlling infectious disease, and understanding the disease's underlying epidemiology is central these efforts. Identification of sources of infection, effective isolation, blockage of possible transmission routes, and protection of the population in a timely manner are all crucial to preventing the spread of infectious diseases. It has been shown that COVID-19 is transmitted through respiratory droplets and contact, and that there is a possibility of aerosol transmission in confined spaces [3]. Further confirmation is needed to verify the presence of fecal-oral transmission of COVID-19 [4]. Mild or asymptomatic patients may not be easily identified; however, these patients can still transmit SARS-CoV-2 to others, posing a substantial challenge for controlling the spread of COVID-19.
Currently, the rapid spread makes COVID-19 a great challenge worldwide. To timely grasp epidemic characteristics of COVID-19, we aimed to perform a retrospective epidemiological study of confirmed COVID-19 cases. Our study findings may be useful to optimize the prevention and control strategies.
Methods
Ethics
The study was conducted in accordance with the requirement of the Helsinki Declaration revised in 2013, and the research protocol was approved by the Ethics Committee of the First Hospital of Jilin University, Jilin Province, China.
Study design
A retrospective cohort study.
Participants
All patients diagnosed with COVID-19 in Jilin Province, China, from January 20 to February 23, 2020 (N = 93) were included in this study.
Data collection
We performed a epidemiological investigation of the 93 included COVID-19 patients. Patients were divided into imported and clustered cases of COVID-19 and further classified based on clinical classification criteria as described in the Diagnosis and Treatment Plan for Coronavirus Disease 2019 (trial edition 7) [5]. We divided the study time period into three time windows (January 20 to 31, February 1 to 10, February 11 to 23) and classified cases based on the final diagnosis. Incubation period was assessed based on the time of last contact or the time the patient left his or her place of residence and the onset time of clinical symptoms.
Study materials and procedure
Patients met diagnostic criteria according to the Diagnosis and Treatment Plan for Coronavirus Disease 2019 (trial edition 7) issued by the National Health Commission and the National Health Administration of the People's Republic of China [5]. Respiratory tract specimens (oropharyngeal swabs or nasopharyngeal swabs) were tested at various local and municipal centers for disease control and prevention in China. Diagnosis of the first case was reviewed by the Jilin Provincial and China Centers for Disease Control and Prevention. Testing was performed using real-time fluorescence-based polymerase chain reaction (PCR) to detect SARS-CoV-2 nucleic acids.
Statistical analysis
All analyses were conducted using SPSS software version 24.0 (IBM SPSS Inc., Chicago, IL, U.S.). The P-P plot method and Shapiro-Wilk test were used to determine normality of variables. Normally distributed variables were presented as mean ± standard deviation ( ± SD). Independent t-tests were used to compare mean age between groups and Wilcoxon signed-rank tests were used to compare median incubation period between groups. Sex distributions were compared using the Fisher's exact test. A P-value < 0.05 was considered statistically significant.
Results
Case severity and age and sex distributions
Among the 93 COVID-19 cases analyzed, there were 15 mild cases (16.13%), 68 moderate cases (73.12%), 6 severe cases (6.45%) and 4 critical cases (4.30%). Patients included 54 (53.76%) males and 39 (41.94%) females, with a mean age was 43.69 ± 17.11 years (range 7 to 85 years) overall, 41.7 ± 15.9 years (range 7 to 85 years) for mild and moderate cases, 55.8 ± 21.3 years (range 24 to 78 years) for severe cases, and 66.8 ± 15.1 years (range 51 to 82 years) for critical cases (Table 1). The age and sex distributions of the included cases are shown in Figure 1. The majority of cases were 20 to 59-years-old (74/93, 79.57%). There were more males than females in most age groups, with the exception of patients < 10-years-old, 10-19, and 30-39 years-old, among whom there were slightly more females than males.
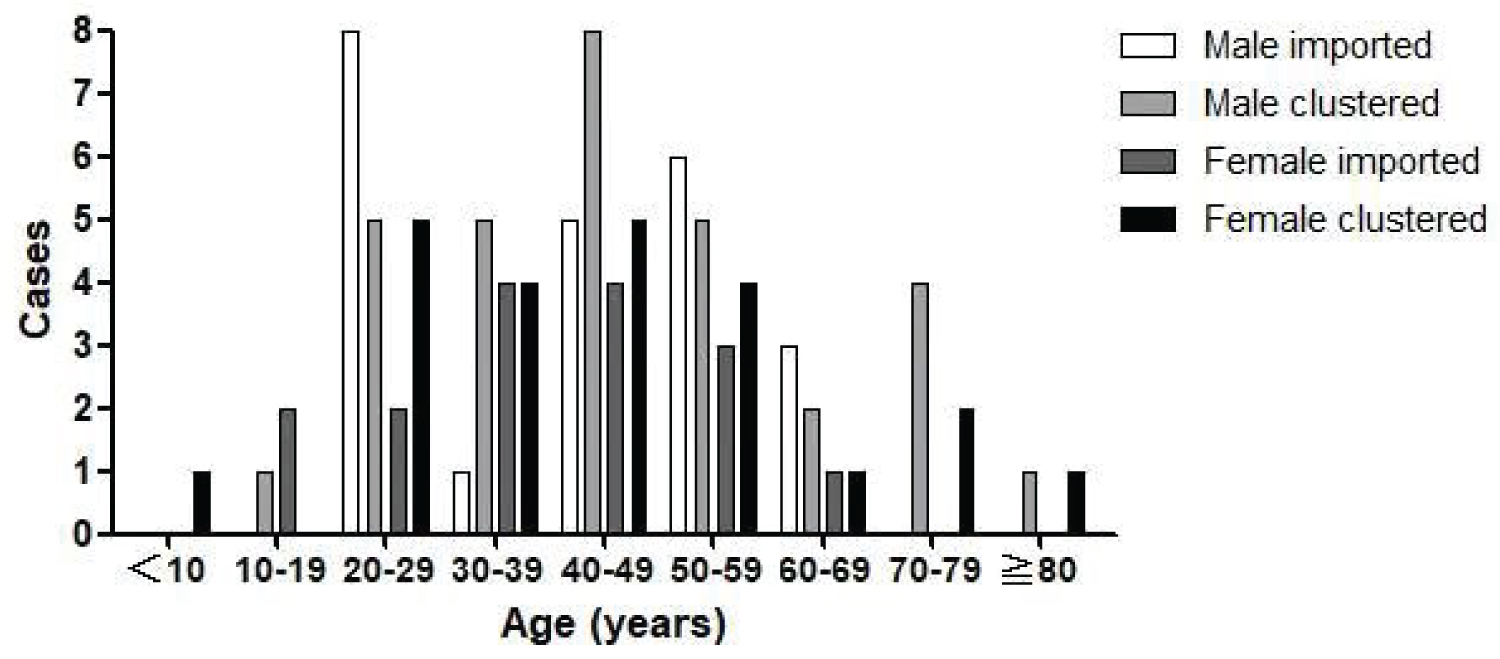
Figure 1: Imported and clustered cases of coronavirus disease 2019 (COVID-19) by age and sex, Jilin Province.
Imported and clustered cases
All 93 patients had studied, worked in, or traveled for business or personal reasons to Wuhan City, Hubei Province; had lived or traveled in other countries or cities (e.g., Thailand, Vietnam, Shandong Province, Guangdong Province, Heilongjiang Province, and Beijing City); or had a history of close contact with a confirmed case from Jilin Province. Among the cases, 39 patients (41.94%) had traveled outside Jilin Province and were classified as imported cases. These included 22 patients (23.66% of cases overall) who had traveled to Wuhan City (the site of the initial outbreak) and 17 patients (18.28%) who had traveled to other provinces or countries (Figure 2). The remaining 54 patients (58.06%) had close contact with a confirmed case and were classified as clustered cases.
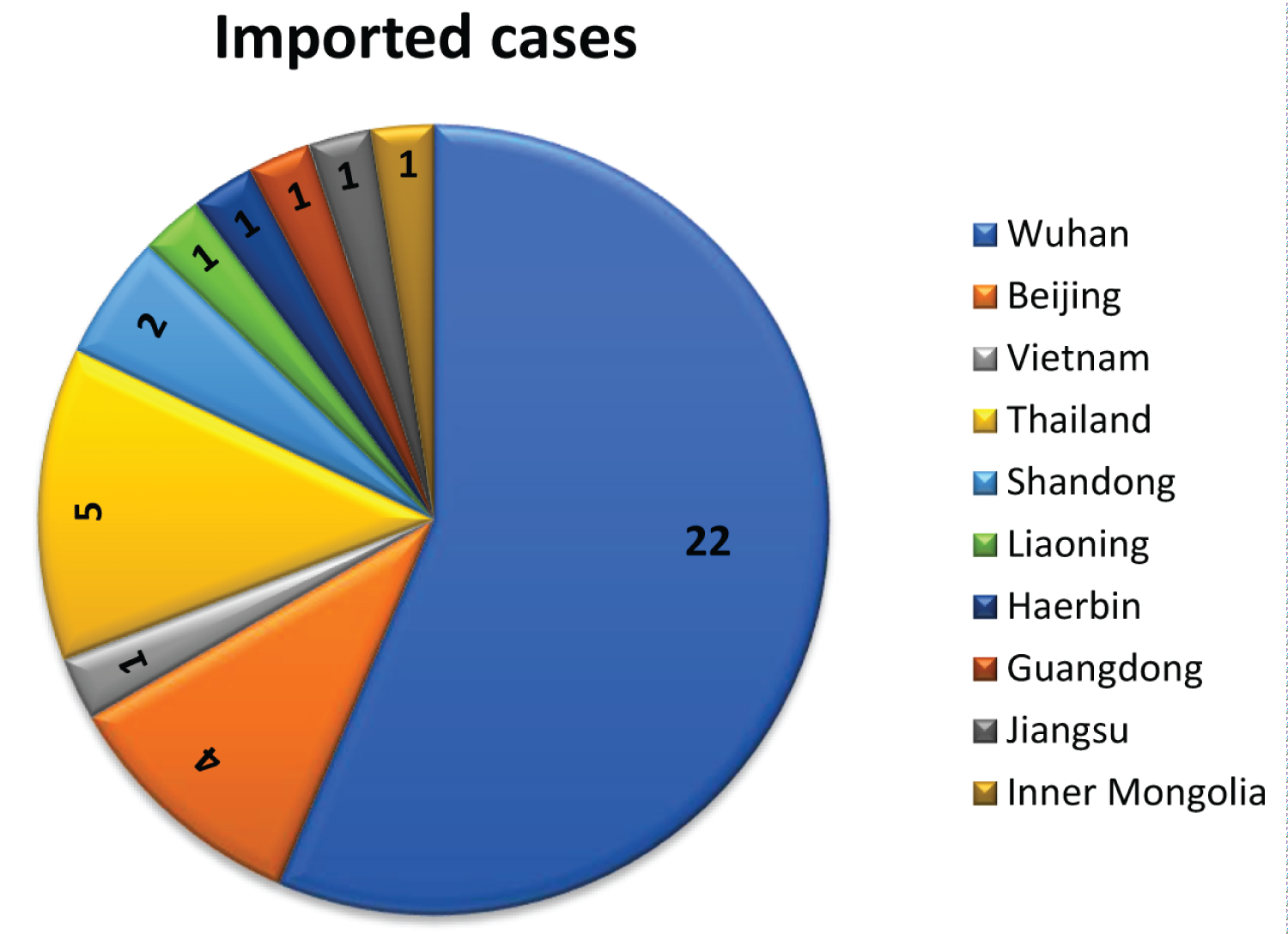
Figure 2: Source of 39 imported coronavirus disease 2019 (COVID-19) cases, Jilin Province.
Age and sex distributions of imported and clustered cases
The distributions of the 39 imported and 54 clustered COVID-19 cases in the three time windows are shown in Table 2. The mean age was 45.57 ± 18.48 years for clustered cases and 41.07 ± 14.84 years for imported cases overall (P = 0.213). The 39 imported cases included 23 males (mean age 43.00 ± 15.51 years, range 21 to 68 years) and 16 females (mean age 38.31 ± 15.33 years, range 10 to 67 years). The 54 clustered cases included 31 males (mean age 46.81 ± 18.05 years, range 17 to 82 years) and 23 females (mean age 43.91 ± 19.32, range 7 to 85 years). Differences in mean age between male and female patients were not statistically significant in either group (P = 0.338 for imported cases, P = 0.574 for clustered cases). Similarly, differences in mean age between imported and clustered cases were not statistically significant among males (P = 0.410) or females (P = 0.340).
Table 2: Imported and Clustered Cases of Coronavirus Disease 2019 (COVID-19) by Time Period and Sex, Jilin Province. View Table 2
The numbers of imported and clustered cases of COVID-19 by age and sex are shown in Figure 1. In the age range of the majority of cases (20-59 years), there were generally more male than female patients among both imported and clustered cases. Exceptions to this pattern is that an equal number of males and females among clustered cases aged 20-29 years.
Occupation distribution of imported cases
Among the 39 imported cases, two people (both males, (Figure 3)) were college students in Wuhan city, eighteen people (eleven males and seven females) worked outside Jilin Province, nine people (four males and five females) had travelled for personal reasons, three people (all males) had travelled for business, and seven people (three males and four females) were migrant workers.
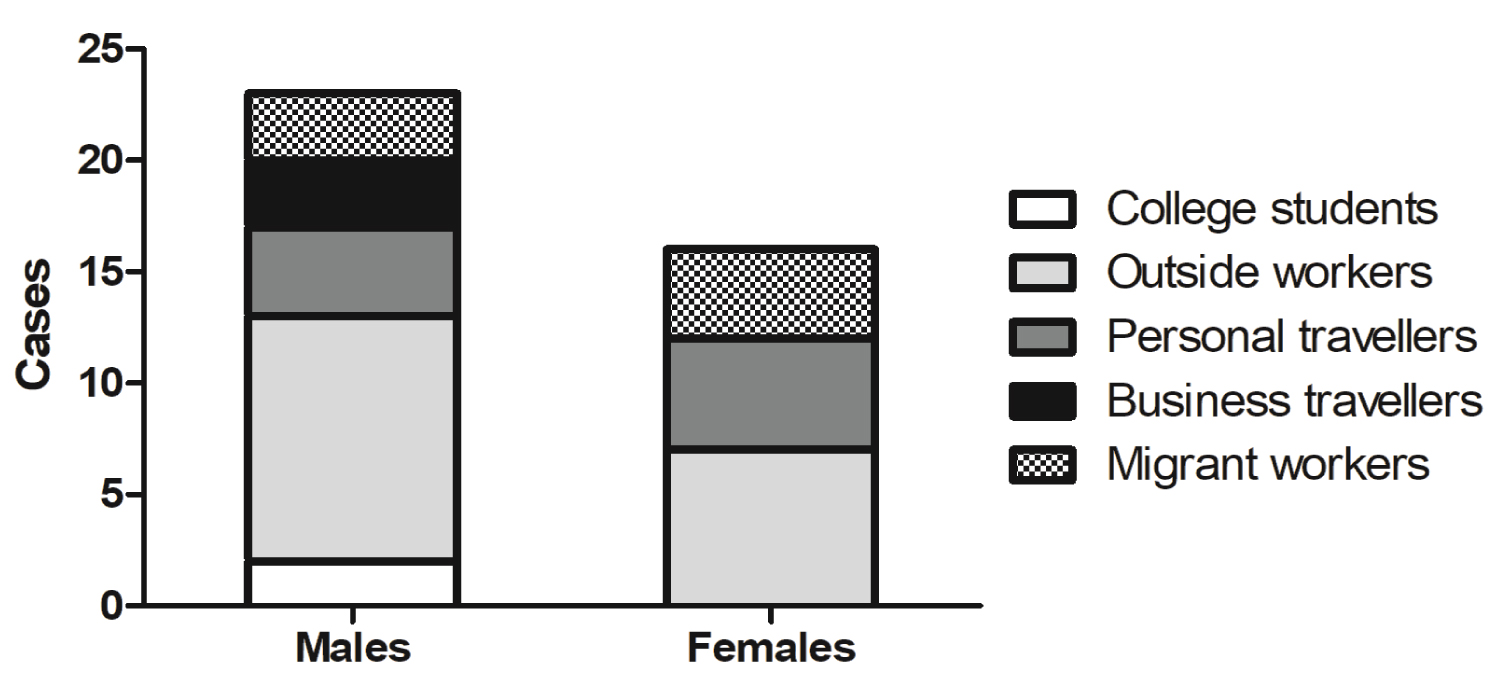
Figure 3: The occupation distribution of imported cases by sex.
Imported and clustered cases by sex and time period
The first and last COVID-19 cases in Jilin Province were confirmed on January 20 and February 23, 2020, respectively. Table 2 shows the number of imported and clustered cases by sex during each of the three time windows we examined within this period. Statistical analysis showed that a significant difference was found in the distribution of imported and clustered cases between the three periods (P < 0.0001). Furthermore, significant difference was found in gender distribution of imported cases (P = 0.0485). Of the 93 patients, nearly 70% (65 cases) were confirmed during the middle time window (February 1-10). During the first time period (January 20-31), 15 imported cases and 2 clustered cases were seen. In contrast, the majority of cases seen during the second time period (February 1-10) were clustered cases (41 clustered cases and 24 imported cases). In the third time period (February 11-23), all 11 cases seen were clustered cases.
Incubation period
Incubation period was accurately assessed in 40 of the 93 patients (28 males and 12 females). The incubation period for imported and clustered cases overall and by sex is shown in Table 3. The median incubation period was 8.0 days (range 1 to 19 days) overall, 7.5 days (range 1 to 15) among males, and 11.0 days (range 3 to 19) among females (P-value for difference between males and females = 0.049). The 28 male patients with a clear incubation period included 14 imported cases and 14 clustered cases, with median incubation periods of 6.0 (range 3 to 13) days and 8.0 (range 1 to 15) days, respectively. The 12 female patients with clear incubation period included 6 imported and 6 clustered cases, with median incubation periods of 9.5 (range 3 to 13) days and 12.0 (range 5 to 19) days, respectively. The median incubation period was shorter for imported cases overall than for clustered cases overall (6.6 days vs. 10.0 days, P = 0.061). Median incubation period did not vary significantly for clustered vs. imported cases among males (P = 0.152) or females (P = 0.195); similarly, differences in median incubation period between males and females were not significant within clustered cases (P = 0.097) or imported cases (P = 0.227).
Table 3: Median Incubation Period of Imported and Clustered Cases of Coronavirus Disease 2019 (COVID-19) by Sex, Jilin Province. View Table 3
Disease severity and outcome
The 93 patients included 83 mild and moderate cases, 6 severe cases, and 4 critical cases. As shown in Table 1, significant difference was found in age distribution between the three groups, and more severe cases tended to be older. However, gender distribution was not found with a significant difference between the three groups (P = 0.5797). Severe and critical cases represented 12.96% of cases among males and 7.69% among females (P = 0.512). Among the 93 cases, 92 patients recovered and one critically ill patient died from COVID-19.
Discussion
As a novel infectious disease, COVID-19 has aroused international concern and interest regarding its epidemiological characteristics. While much remains to be clarified, progress has been made in understanding the underlying disease characteristics and patterns of transmission.
Individuals generally lack immunity to novel infectious diseases and are thus highly susceptible, and SARS-CoV-2 is more contagious than severe acute respiratory coronavirus (SARS-CoV) and middle east respiratory syndrome coronavirus (MERS-CoV) [6]. We found that the majority of COVID-19 patients in Jilin Province were men, 41.94% were females, this is consistent with the report from 1099 patients in mainland China [7], though the proportion of men declined across the study period. A substantial portion of patients were also originally from other provinces (predominantly Hubei Province, site of the initial outbreak). These patients were mostly working or travelling for business purposes, which explains the predominance of men. In addition, 80% of COVID-19 patients were between the ages of 20 and 59 years and thus may have had more opportunities for social gatherings and greater likelihood of contact with sources of infection. A large epidemiological study of 44,672 confirmed COVID-19 cases led by the China Center for Disease Control and Prevention (CDC) found that 86.6% of the COVID-19 patients were between the ages of 30 and 79 [8]. In our study, 72.04% of patients (67/93) were in this age range, while nearly 20% (20/93) of imported and clustered cases occurred in young adults aged 20-29 years. Of the eight patients aged 70 or above in our study, all were clustered cases who had a history of direct contact with relatives returning from Wuhan. Four of the seven patients aged 60-69 had a history of close contact with a confirmed case, and the remaining three patients had travelled to Wuhan or to other countries. Fifty-six percent of the imported cases in Jilin were from Wuhan, the site of the initial outbreak and an area of high incidence during the early stages of the epidemic.
Analysis of the incubation period of COVID-19 patients in Jilin Province showed an overall median incubation period of 8 days, while the median incubation period of female patients was 3.5 days longer than that of males. There did not have reports about the gender differences of the incubation period between males and females to COVID-19, but a publication indicated that seven of nine COVID-19 infant patients were females [9], and SARS-CoV has also been found to infect more males than females [10]. Further research is needed to confirm whether females having stronger antiviral immunity than males, and if so, why.
In our study, the shortest incubation period was 3 days in female patients and 1 day in male patients; the longest incubation period was 19 days in a female patient, who had mild clinical symptoms but clear pneumonia lesions in her chest computed tomography (CT). Several other studies have also found COVID-19 incubation periods exceeding the commonly-used standard of 14 days. Although the exact incubation period could be traced in fewer than half of the cases in our study, we were able to trace the incubation period on a sizable sample of imported and clustered cases among both males and females, suggesting that incomplete tracing of incubation period is not likely to be a source of bias. An epidemiological analysis of 483 COVID-19 cases in Henan Province found that 7.45% of patients had an incubation period greater than 14 days [11], while a study of 73 patients in the surrounding areas of Wuhan, Hubei Province found a maximum incubation period of 26 days [12]. Accordingly, we recommend that the standard maximum incubation period of 14 days be further verified in large-sample studies.
Understanding the incubation period of COVID-19 is essential for tracing sources of infection and determining transmission routes, optimal length of hospital stay, and duration of quarantine and medical observation of close contacts. The observed incubation period differs between studies, as does the maximum incubation period. Most studies do suggest that the incubation period of COVID-19 is generally less than 14 days, with observed median incubation periods ranging from 3 to 7 days. Two studies found an average incubation period of 5.2 days. One of these was a retrospective analysis of 10 cases during the early period of the outbreak conducted by the China CDC. In that study, 95% of patients had an incubation period < 12.5 days [13]. The other was a study of 101 confirmed cases from 38 provinces, territories or countries, in which 97.5% of patients had an incubation period < 11.5 days [14].
Knowledge of the incubation period of a disease enables prediction of approximate disease onset time after viral infection. The COVID-19 epidemic began slightly later in Jilin Province than in some other parts of China, and there was an interval of one month between confirmation of the first and last cases in Jilin. Analysis of cases over the course of that one-month period showed that imported cases were predominant during the first 10 days, which is consistent with the disease course of COVID-19. Most patients who had worked or traveled outside of Jilin returned to the province before the lockdown of Wuhan City on January 23, 2020. Given that the incubation period is most frequently between 3 and 7 days [5], some of the imported cases had appeared before January 31, 2020, and these cases were already infectious before onset and diagnosis. Therefore, as some patients had a relatively long incubation period or other family members who had been infected and developed the disease, a peak onset period of imported and clustered cases occurred from February 1 to 10, during which nearly 70% of overall COVID-19 cases in Jilin Province were diagnosed. During the last 13 days of the epidemic in Jilin, all cases were clustered cases. This pattern is consistent with the development, progression, and outcome of the COVID-19 epidemic in other locations. A study conducted at the Fifth Medical Center of Chinese People's Liberation Army (PLA) General Hospital found that more than 30% of COVID-19 cases (n = 26) arose from familial clustering [15]. In our study, more than half of patients (54/93 or 58.06%) were clustered cases, a significantly higher proportion than found in previous studies. This discrepancy may be related to the fact that Jilin province is an agricultural province with less-developed tourism and fewer migrant workers than major cities in China such as Beijing, leading to relatively fewer imported cases and more clustered cases than in those cities. In addition, because of the substantial incubation period of COVID-19, it is likely that imported cases had contact with others and may have infected family members, relatives, or friends before the onset of clinical symptoms and quarantine. The incidence of clustered cases in Jilin was relatively high, emphasizing the importance of timely isolation of individuals with a history of possible exposure through personal contact in affected areas.
The proportion of COVID-19 patients in Jilin Province who were male fell from 82.35% at the end of January 2020 to 54.55% in the middle of February. This pattern may result in part from the longer incubation period of COVID-19 in female patients.
The majority of COVID-19 cases tend to be mild and moderate [5]. In the present study, 89.25% of patients had mild-to-moderate COVID-19, and 6.45% and 4.3% of patients had severe and critical COVID-19, respectively. These figures are similar to those from a previous study of 44,672 confirmed COVID-19 cases in which 80.9% of patients had mild-to-moderate COVID-19, 13.8% had severe COVID-19, and 4.7% had critical COVID-19, with a mortality rate of 49% among critical cases [8]. A WHO report also noted that approximately 14% of COVID-19 patients had severe disease, that 5% of patients needed to be treated in an intensive care unit, and that advanced age and comorbidities were the strongest risk factors for mortality [16]. In our study, severe and critical cases were substantially older than mild-to-moderate cases, corroborating earlier findings that advanced age is associated with greater disease severity in COVID-19 patients [17]. The proportion of severe and critical cases was slightly higher among males than among females (12.96% vs. 7.69%). One study patient died, an 82-year-old male with a history of cerebrovascular disease, hypertension, and cryptogenic organizing pneumonia. It is consistent with the results that SARS-CoV-2 is more likely to infect older adult males with chronic comorbidities [17]. His disease course from onset to death lasted 12 days, suggesting that severe cases develop dyspnea and/or hypoxemia approximately one week after disease onset, and that the most severe cases may rapidly progress to acute respiratory distress syndrome and septic shock [18]. Accordingly, it is crucial that health care providers pay close attention to changes in disease condition for patients at these stages. Further research is needed to verify how the speed and course of disease progression in COVID-19 may vary between males and females.
The key to stopping a severe infectious disease epidemic is prevention and control rather than treatment per se. Better understanding of the epidemiological characteristics of the disease will help to improve prevention and control and thereby reduce disease incidence. Echoing such appeals, on February 19, 2020, the New England Journal of Medicine once again called for urgent evidence from epidemiological investigation of COVID-19 [19]. Although our study has well documented the issue, a short study period should be considered as a limitation when interpreting the finding. This is because a long study period could provide more details on the patient changes over time.
In summary, while the entire population is susceptible to COVID-19, contracting the disease requires contact with a source of infection. Hence, tracing the history of exposure to confirmed cases and the history of travel to affected areas is crucial. Given the presence of COVID-19 cases with incubation periods exceeding 14 days, it is necessary to revise our understanding of the disease's incubation period, especially for female patients, who may have a longer incubation period. Revising protocols for clinical care of COVID-19 is also advisable, including possibly extending of the observation period for suspected cases from 2 to 3 weeks.
Declarations
Funding
This work was supported by the Emergency Scientific Research Fund for the Prevention and Control of Novel Coronavirus Pneumonia of the Science and Technology Department of Jilin Province [grant number 20200901008SF]. The authors declare that they have no financial relationship with the organization that sponsored the research, and the funding body was not involved in study design, data collection, analysis and writing of the study.
Competing interests
The authors declare that they have no conflict of interest.
Availability of data and materials
The datasets generated and analyzed during the present study are available from the corresponding author on reasonable request.
Authors' Contributions
Kai-yu Zhang and Yang Wang designed/performed most of the investigation; Cai-xia Liu, Lu-yao Sun performed the data analysis and wrote the manuscript; Dan-ping Peng contributed to interpretation of the data and analyses. All of the authors have read and approved the manuscript.
Ethics Approval and Consent to Participate
The study was conducted in accordance with the requirement of the Helsinki Declaration revised in 2013, and the research protocol was approved by the Ethics Committee of the First Hospital of Jilin University, Jilin Province, China. Written informed consent was obtained from all individual participants included in the study.
Consent for Publication
All data published here are under the consent for publication. Written informed consent was obtained from all individual participants included in the study.
Acknowledgements
Not applicable.
References
- Organization WH. Situation report – 22: Novel coronavirus (2019-nCoV).
- Zhou M, Zhang X, Qu J (2020) Coronavirus disease 2019 (COVID-19): A clinical update. Front Med 14: 126-135.
- Association SEGfCotEoNCPotCPM (2020) An update on the epidemiological characteristics of novel coronavirus pneumonia (COVID-19). Zhonghua Liu Xing Bing Xue Za Zhi 41: 139-144.
- Zhang W, Du RH, Li B, et al. (2020) Molecular and serological investigation of 2019-nCoV infected patients: Implication of multiple shedding routes. Emerg Microbes Infect 9: 386-389.
- China NHCotPsRo. The diagnosis and treatment plan for coronavirus disease 2019 (trial edition 7).
- Wang C, Horby PW, Hayden FG, et al. (2020) A novel coronavirus outbreak of global health concern. Lancet 395: 470-473.
- Guan WJ, Zheng yi Ni, Yu Hu, et al. (2020) Clinical Characteristics of Coronavirus Disease 2019 in China. N Engl J Med 382: 1708-1720.
- Epidemiology Working Group for NCIP Epidemic Response CCfDCaP (2020) The epidemiological characteristics of an outbreak of 2019 novel coronavirus diseases (COVID-19) in China. Zhonghua Liu Xing Bing Xue Za Zhi 41: 145-151.
- Wei M, Yuan J, Liu Y, et al. (2020) Novel Coronavirus Infection in Hospitalized Infants Under 1 Year of Age in China. Jama 323: 1313-1314.
- Channappanavar R, Fett C, Mack M, et al. (2017) Sex-Based Differences in Susceptibility to Severe Acute Respiratory Syndrome Coronavirus Infection. J Immunol 198: 4046-4053.
- Wang P, Lu J-A, Jin Y, et al. (2020) Statistical and network analysis of 1212 COVID-19 patients in Henan, China. Int J Infect Dis 95: 391-398.
- Zheng Y, Xiong C, Liu Y, et al. (2020) Epidemiological and clinical characteristics analysis of COVID-19 in the surrounding areas of Wuhan, Hubei Province in 2020. Pharmacol Res 157: 104821.
- Li Q, Guan X, Wu P, et al. (2020) Early Transmission Dynamics in Wuhan, China, of Novel Coronavirus-Infected Pneumonia. N Engl J Med 382: 1199-1207.
- Lauer SA, Grantz KH, Bi Q, et al. (2020) The Incubation Period of Coronavirus Disease 2019 (COVID-19) From Publicly Reported Confirmed Cases: Estimation and Application. Ann Intern Med 172: 577-582.
- Jie ZY, Zhu C, Jin L, et al. (2020) Clinical and epidemiological characteristics of 26 patients diagnosed with COVID-19. Zhonghua Yi Yuan Gan Ran Xue Za Zhi 30: 826-829.
- WHO (2020) Clinical management of severe acute respiratory infection (SARI) when COVID-19 disease is suspected: Interim guidance.
- Chen N, Zhou M, Dong X, et al. (2020) Epidemiological and clinical characteristics of 99 cases of 2019 novel coronavirus pneumonia in Wuhan, China: a descriptive study. Lancet 395: 507-513.
- Wang D, Hu B, Hu C, et al. (2020) Clinical Characteristics of 138 Hospitalized Patients With 2019 Novel Coronavirus-Infected Pneumonia in Wuhan, China. JAMA 323: 1061-1069.
- Lipsitch M, Swerdlow DL, Finelli L (2020) Defining the Epidemiology of Covid-19 - Studies Needed. N Engl J Med 382: 1194-1196.
Table 1: Age and Sex Distribution of Coronavirus Disease 2019 (COVID-19) Cases by Clinical Classification, Jilin Province. View Table 1